

Trick or Treat? Role of Uric Acid and Central Obesity On the Risk of Metabolic Syndrome
Mendelian randomization showed uric acid may raise the risk of metabolic syndrome (MetS) by raising blood pressure & triglycerides while lowering HDL-C but not by accumulating fat or hyperglycemia. High waist circumference may be causal for all the components of MetS, even hyperuricemia.
Mendelian randomization showed uric acid may raise the risk of metabolic syndrome (MetS) by raising blood pressure & triglycerides while lowering HDL-C but not by accumulating fat or hyperglycemia. High waist circumference may be causal for all the components of MetS, even hyperuricemia.
By: Institute of Biomedical Sciences, Academia Sinica
Metabolic syndrome (MetS) is a collection of conditions that happen together, increasing your risk of heart disease, stroke, and type 2 diabetes. These conditions include increased blood pressure, high blood sugar, excess body fat around the waist, and abnormal cholesterol or triglyceride levels.
Metabolic syndrome predicts not only the risk of developing diabetes, cardiovascular diseases, and chronic kidney disease but also that of many degenerative diseases in later life.
Although both cross‐sectional and longitudinal studies have implicated that abdominal obesity is the central feature of this complex condition, the pathogenesis of MetS is very complex in terms of the underlying mechanism, the sequence of development, and the interactions among individual components and with other metabolic disorders.
According to Dr. Wen-Harn Pan “We noticed that Taiwanese experience almost the highest prevalence of hyperuricemia in the world. We would like to know more about its impacts than just gout. Our previous cohort studies found hyperuricemia as a strong predictive factor on cardiovascular diseases (CVD) and urate-lowering treatment can lower CVD incidence. Furthermore, our earlier Mendelian Randomization study in Han Chinese confirmed that genetically exposed to high blood uric acid increased the risk of CVD events”
It is generally accepted that central obesity is a core component of metabolic syndrome. On the other hand, hyperuricemia, the predecessor of gout, has been found to cluster with multiple components of MetS. But it is unclear whether hyperuricemia is a downstream result of central obesity/MetS or may play an upstream role in MetS development.
Elevated serum uric acid (SUA) has been associated with increased blood pressure, body mass index, triglyceride, and reduced HDL-C. Hyperuricemia also predicts the development of MetS, insulin resistance, hypertension, and diabetes.
Nonetheless, so far hyperuricemia has not been included as a component of the syndrome MetS. A comprehensive map of such a complex syndrome will help form strategies for prevention and management.
To address this question, researchers at the Institute of Biomedical Sciences, Academia Sinica has carried out a study using 10,000 participants from Taiwan Biobank. The aim of the TWB is to establish a population-based database, gathering information from 200,000 volunteers on genetic, lifestyle and environmental factors.
Recently Dr. Pan and her colleagues at IBMS and IIS at academia Sinica discovered that the peak age of onset for hyperuricemia occurs earlier than those of hypertension and diabetes in a Taiwanese cohort study. Based on this they hypothesized that uric acid may have a causal relationship with the components of MetS.
“As hyperuricemia and obesity are preventable, our findings are of relevance to public health policy and practice, and uric acid control can be prioritized to the same extent as obesity, dyslipidemia, and hypertension” Says Dr. Mahantesh Biradar
In this regard, a Mendelian randomization (MR) study was conducted by analyzing data from a total of 10,000 participants of the Taiwan Biobank (TWB). MR technique exploits the random distribution of genetic variants at the gametogenesis phase, enabling their use as instrumental variables for testing the causality and is less likely to be affected by confounding or reverse causation than conventional observational studies.
The investigation shows that uric acid increment may augment the risk of MetS through increasing blood pressure and triglyceride levels and lowering HDL-C value but not through accumulating fat or hyperglycemia. High waist circumference may be a causal agent for all the components of MetS including hyperuricemia. Moreover, their MR study results support the idea that hyperuricemia may play a causal role in cardiovascular disease development.
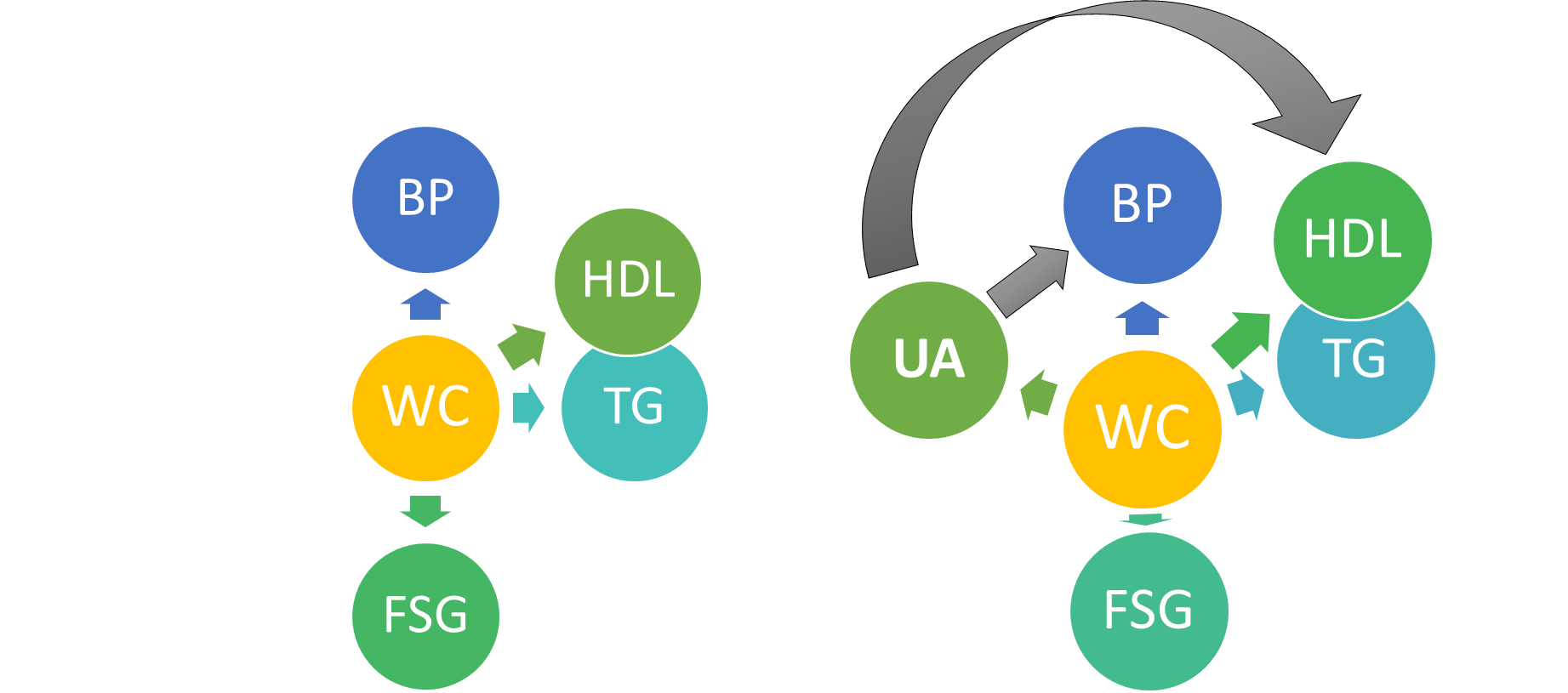
In other words, the study shows that genetic predisposition to higher levels of uric acid is causally associated with blood pressure elevation and dyslipidemia components of MetS, but not obesity/diabetes components, suggesting that SUA may involve a separate pathway of MetS development independent of obesity.
Findings like these may alter clinical thinking such that control of uric acid can be prioritized to the same extent as obesity, dyslipidemia, and hypertension. Whether hyperuricemia may be considered as a therapeutic target for preventing MetS warrants further studies. The findings from this study have been published in the International Journal of Obesity.





Leave a Reply